We’ve all heard the term “survival of the fittest,” which scientist Charles Darwin famously coined to explain how organisms with heritable traits that give them an advantage — such as avoiding predators or beating out others for the chance to mate — are able to survive and pass on these advantageous traits to their offspring.
In his talk with ClubEvMed last Tuesday, Brian Hare of Duke Evolutionary Anthropology explained key points from his new book that he co-authored with his wife and research partner, Vanessa Woods, entitled Survival of the Friendliest: Understanding Our Origins and Rediscovering Our Common Humanity.
Image from Penguin Random House
The term “fittest” is often associated with animals who are physically stronger or of more value than others, but being “fit” can also include an organism’s ability to communicate well with others in its group, which can provide an evolutionary advantage. For example, more social animals can form alliances with each other and protect each others’ young, so the whole population stays stronger in terms of number.
Hare cited a comparison between chimpanzees and bonobos, both of which have the potential for infanticide by aggressive males in a group. However, bonobos have zero cases of infanticide because female bonobos are able to communicate well and form alliances to protect each others’ young from aggressive males. Since the high cost of aggression for males outweighs the benefit, the males are friendlier, and the young bonobos survive. While this is a specific case with wild animals, other species have adopted social skills as a method of survival through domestication or self-domestication.
Image from brianhare.net
Hare referred to dogs as “exhibit A” of survival of the friendliest via domestication, because humans have bred dogs that are more playful, approachable and patient for centuries. Dogs are exceptionally good at understanding, responding to and communicating with humans as a result of domestication. Hare also explained one Russian study in which they began selecting foxes based on their friendliness towards people. They bred the most friendly foxes together and then compared the friendliness of their offspring to the offspring of randomly bred foxes. The results showed that friendlier foxes differed in physiology in addition to behavior, and were better at cooperating and communicating with humans. This is an example of self-domestication, which changes development patterns and has increased fitness via friendliness. Friendliness in this case means skill in cooperating and communication.
Survival of the Friendliest argues that humans today are the friendliest species of human, which may be why we have lasted so long evolutionarily. However, with the new type of friendliness also comes a new type of aggression. Mother bears are kind and nurturing to their cubs, but also have the most potential for aggression when they feel their cubs are threatened. Similarly in humans, when we feel people who share our identity are threatened, we want to protect those individuals.
Hare and Woods reason that this desire to protect also reduces our ability to cooperate or communicate with those who we feel threaten us or threaten our “group”— whether this be our family, our race or another trait. When our ability to communicate is reduced, we begin to dehumanize those who we feel threaten the people who share our identity. This then becomes a cycle, where people dehumanize those who they believe are dehumanizing them.
In order to stop this cycle, Hare and Woods argue that humans will need to alter their view of who they believe “belongs” to their group to include more people. We need to communicate openly and build a desire to protect other humans, rather than dehumanize them.
After my freshman fall, I swore I’d never take another 8AM class. Yet, when a microbiology lab was the only opportunity I had for an in-person course in Duke’s disrupted Fall 2020 semester, I jumped at the chance to take it. Wednesdays have become my on-campus days, and though they start at 7AM and are often jam-packed until 7PM, they are my favorite days of the week.
I’m usually the first to arrive in sub-basement of the Biological Sciences building on Wednesdays. As my six lab-mates join me, we stand in line on top of stickers spaced according to 6-foot social-distancing guidelines and talk about questions from class or the lab we’re going to perform that day. Sometimes it’s difficult to hear one another through our masks. When our TA is ready for us to enter the classroom, we do so one at a time, only after she’s verified our Symptom Monitoring status and taken our temperature.
Stickers marking 6-ft distances for safety. The lab layout with seating arrangements according to Covid guidelines.
Our lab stations are spaced so that we are appropriately distanced from one another, but able to work and collaborate as a team as best we can. We have a no-contact drop-zone for placing and picking up shared lab items, though each students’ space is equipped with most everything we need for our lab on most occasions. The stations are close enough so that we can chat, compare results, and ask each other for assistance as we work. Everyone wears a face shield over a face mask. Each lab session we exchange our “home” face mask for a disposable “lab” face mask. Since we work with potentially pathogenic microbes, this step is for our safety to make sure we don’t carry harmful bacteria out of our lab space. Unlike previous years, gloves are worn at all times, but the lab coats we wear have always been a standard part of the microbiology lab attire.
The infamous “no contact drop zone” for use of shared materials during lab.
What used to be two, two-hour lab sessions twice a week has been condensed into a single four-hour lab-session to minimize exposure to one another. At the beginning of the semester it felt strange and uncomfortable to wear a mask for the whole lab period and for the rest of the day on campus. But like many changes due to Covid-19, I’ve simply gotten used to it. It’s worth it to have face-to-face interactions with fellow students and to have hands-on experience in the lab. In many ways, these experiences feel much more real and meaningful than my fully online classes, in which I interact exclusively virtually with peers and instructors.
This semester we’ve also been doing science at home, having been tasked with an independent research project to be performed outside of lab. The kitchen in my apartment has become a makeshift space for inoculating TSA plates and perplexing my roommate with my experiment.
At home experimental set-up and data collection in my apartment.
After microbiology, I grab a quick lunch at West Union…which I’m still figuring out how to navigate. There’s more online ordering and different routes for lines I haven’t gotten used to. Though it’s significantly less crowded than it used to be – which has its advantages – the energy and fervor that made up Duke is certainly missing. Though I feel it in spurts when I run into the rare upperclassman on the Plaza or in the Bryan Center while trying to find a spot to study, campus is unequivocally not the same.
I leave the central part of campus and return to the basement of BioSci to work in my research lab, the Steve Nowicki Lab. According to our Covid plan, a grad student must be present to supervise me at all times and each of us works on opposite sides of the lab space. It’s really not all that different than it used to be.
In the Nowicki Lab, I test the categorical color perception of Zebra finches. After being trained for the trials, the birds are tested to see if they can detect color differences between a background color and two “odd color out” chips. Colors one and eight are most starkly different, but when comparing colors seven and eight, for example, I sometimes struggle to tell the two colors apart.
Background color 8 versus odd-color-out 7. Can you tell the difference? (Color 7 is in wells 1 and 7)
Following a five-month hiatus from running trials, I was pleasantly surprised to find myself in the rhythm of things with only a few marginal mishaps. Within a half-hour of being back in the lab, I was running experiments at full speed again. For a moment it felt like I’d never left, and like it could have been the Wednesday before spring break, before the pandemic took full effect. Sometimes still when I’m running trials, I imagine I could walk out of BioSci’s basement and find that everything would be just as it had been when I left in March.
I spend three hours with the birds, running a refresher round followed by five experimental trials. And usually, I listen to podcasts while I work. The time passes quickly, sometimes more quickly than I’d hope.
Example of bird during experiments.
Since I’m already on campus, most Wednesdays I stick around and attend my online history seminar from a spot around campus. Though I can’t perch myself on the third floor of Perkins Library these days, I’ve found a new spot I like on the second level of the Bryan Center and I’ve made it work for me.
On Wednesdays, I am reminded of the reasons I fell in love with Duke and of all the things I miss about it in these strange and uncertain times. I wonder if the Duke I knew will ever be the same. Or if something has fundamentally shifted in our institution, and more largely in each of us individually, that only leaves us with a path forward to a new Duke, rather than a return to the old.
I am team Crystal Violet #2 and this is my bag for placing my “home mask” in when gearing up for lab.
As I return to my car in Blue Zone, I take a longing look at the Chapel. Then I make my way to my car, turn on some tunes for the drive home, and patiently wait for my alarm to wake me at 7AM the next Wednesday morning.
Most of the time I’m left thinking about the Duke that used to be, despite the fact that I certainly admire the socially-responsible and safe Duke that is. We’re doing well, all things considered. But still, it’s not the same. The Duke that the first years know is not the Duke I remember.
Who will be the first company to secure an Emergency Use Authorization for a Covid-19 vaccine, and when? This question has circulated in the popular press for a few months and is at the forefront of many Americans’ minds with the upcoming presidential election on November 3rd.
Arti K. Rai (J.D.) moderated a dialogue between former FDA Commissioner and distinguished Professor of Cardiology, Robert Califf (M.D., M.A.C.C.), and Founder and Director of Scripps Research Translational Institute, Eric Topol (M.D.), in which the pair discussed emergency use authorization, public trust, and vaccines. The discussion was part of the Science & Society Initiative’s ongoing series of “Coronavirus Conversations.”
Arti Rai (J.D.)
Robert Califf (M.D., M.A.C.C.)
Eric Topol (M.D.)
Left to right: Moderator Arti Rai and Panelists Robert Califf and Eric Topol
Emergency Use Authorizations (EUAs) strengthen American public health protections by speeding the availability and use of medical countermeasures during public health emergencies. Dr. Califf explained that in addition to events like nuclear catastrophes that EUAs were designed to provide protections for, pandemics were also thought about in conceiving the emergency measure. “[The pandemic] is not a surprise,” Califf said, “We knew it was going to happen at some point.”
The panelists examined the possible use of EUAs for a Covid vaccine and monoclonal antibody treatments given the EUAs issued earlier this year for hydroxycholoroquine and convalescent plasma, the former of which was revoked due to proven risks. Both of these experimental treatments lacked sufficient evidence at the time the EUAs were approved.
Dr. Topol said that the EUA case for the antibodies treatment is a good one with growing evidence that suggests their effectiveness as a viable treatment measure. Dr. Califf concurred, saying that with 1,000 people predicted to die every day in the U.S. through the end of December, there’s a strong case for the FDA to exert its judgment. One issue with antibodies, however, is that they cannot be made in large quantities and are very expensive, meaning they would be inaccessible for many.
The question of EUA use for vaccines is less straightforward. Dr. Topol argued that though the protocols released by four drug companies, including Moderna and Pfizer, are pretty far along, “there is a very questionable ethical story here.” He continued, “How can we say it’s good enough to give to essential workers, healthcare works, high-risk individuals, but they won’t even give it to trial participants? They received placebo vaccines.” Across the board, the trials currently underway only include about 150 individuals.
These initial trials are only the first hurdles to the production of a vaccine, according to both Califf and Topol. Dr. Califf pointed out that there will be issues of manufacturing and distributing, lots of concerns with post-market assessments, and how to determine which vaccines will be the best. Dr. Topol reinforced these ideas, suggesting that because no single company will be able to fill the vaccine demands, we need multiple vaccines to be successful. Further, Dr. Topol admitted his concern about the major extrapolations of data we will face, going from trials of 150 individuals to potential distribution numbers of vaccines reaching the hundreds of millions, if not billions of people.
And even once an initial round of vaccines is developed, Dr. Califf inserted the question, “What happens after people get vaccinated?” The simple truth is, the vaccination will probably not completely eradicate the virus, there could be late post-vaccination reactions, and the vaccine could potentially end up creating asymptomatic carriers. Both doctors agreed, masks and social distancing will be needed for at least the next year.
The potential of a Covid-19 vaccination has been popular in the media over the last few months.
Public opinion and politics are also key players in vaccine debates and development. “The point of public trust is essential because if something happens with the first vaccine that gets out,” Dr. Topol said, “it’s going to be a real damaging blow to vaccine rollout.” Like mask-wearing, Topol suggested that vaccines are part of a larger social contract in which these sorts of preventative measures not only help oneself but those around them.
Rai pointed out that as tensions between the FDA and the U.S. department of Health and Human Services grow, as well as between the FDA and the Trump administration, we could face “doomsday” scenarios where the FDA is coerced into certain actions and their powers become limited. However, new FDA guidelines for vaccine development have extended the potential timeline for a Covid vaccine, meaning that the chances of a EUA being issued before the election and being utilized as a political tool for Trump’s reelection are quite unlikely at this point.
Dr. Califf closed by emphasizing the need for solidarity among the biomedical community as influential to the success or failure of potential vaccines and public trust. Dr. Topol offered that we “need education, government that supports science, and need to get [support from] people of all diverse backgrounds to get [the public] to buy in.”
While Dr. Topol maintained a more skeptical and sometimes grim tone, Dr. Califf said that though he’s worried about “everything,” he’s “preparing for the worst but hoping for the best.”
It seems that as many people grow both accustomed to and tired of our new normal, most of us are caught somewhere in the middle of these outlooks.
Conversations on and actions toward making American medicine less racist continue to grow. At Duke, that includes looking at our own history as a hospital and medical center serving a diverse community.
In a Sept. 22 virtual conversation, Duke physicians Damon Tweedy M.D., Associate Professor of Psychiatry and Behavioral Sciences, and Jeffrey Baker M.D., Ph.D., Director of the Trent Center for Bioethics, Humanities, and History of Medicine, spoke about the history of Duke’s legacies of race and memory. (Watch the presentation here.)
The career of Dr. Baker, who is a professor of both pediatrics and history, has taken him around the globe, right back to his hometown of Durham –where he said he has found the most interesting story of all.
After becoming Director for the Trent Center in 2016, he was approached with “hunger” by Durham natives to know their hometown’s story. Through oral and archival sources, Dr. Baker has broached Duke hospital’s history with humility in hopes of uncovering and contextualizing the historical roles of race in Duke medicine and Durham.
Dr. Tweedy, author of Black Man in a White Coat, attended Duke for medical school in the 1990s. He was warned that it was a plantation and an institution built on tobacco and slave money.
Though Dr. Baker proposed that in many ways the hospital structure often reflects plantation hierarchies in which there is racialization of who holds what jobs and power, he said Duke’s endowment money actually came from technological progress within tobacco production rather than slavery or plantations directly.
The Duke family’s vision for the hospital was quite different from actual outcomes in practice, Dr. Baker said. The Dukes were considered racial progressives in their time and the endowment they provided to launch the Duke Medical School and Hospital in 1930 was meant to improve health and education in North Carolina and train primary care doctors for the state.
“However,” Dr. Baker said, “there were two realities: Jim Crow and the Great Depression.”
Dr. Tweedy and Dr. Baker via Zoom
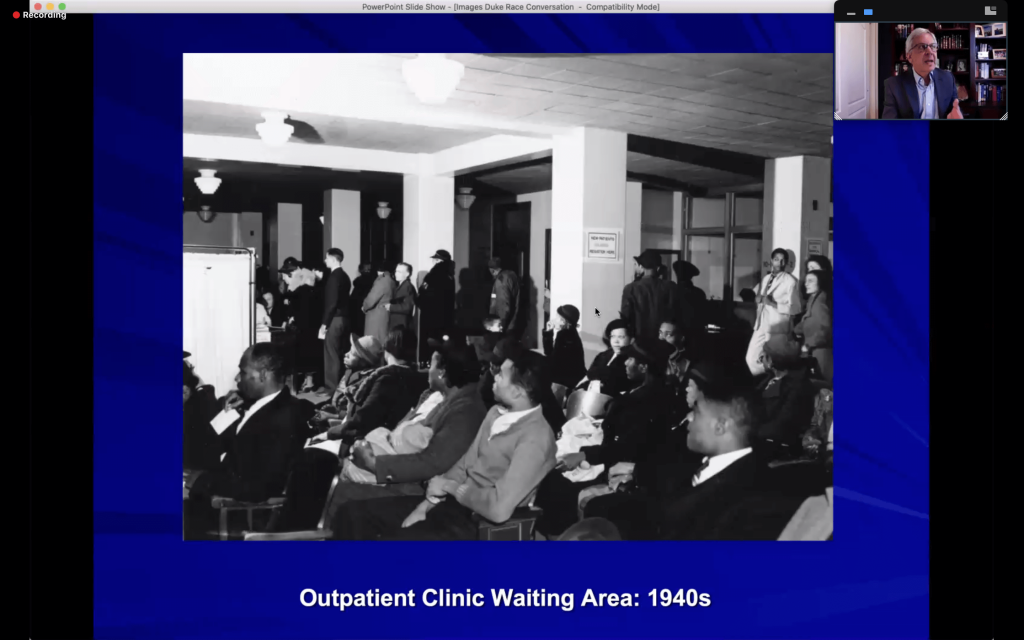
During the era of Jim Crow segregation, Duke’s primary care doctors were all white, and nearly all male. Though the hospital cared for both Black and white patients, they were segregated by race. Black patients had separate wards, and waiting areas for pediatric care were separated racially by days of the week. Waiting areas for adult patients functioned without appointments, but only white people were seen before noon. It’s likely that the care granted to white people in the first half of the day was superior to that of Black people receiving care at 4 pm or told to return the next day, he said.
Original floor plans for the Duke Hospital.
The Great Depression also generated a diversion from plans in the 1940s. When the Duke Hospital came close to bankruptcy, it chose to open private clinics on the side for revenue – which had an unintended consequence. The clinics brought a lot of money into Duke, Dr. Baker said, but it also reinforced distinctions between those who could pay for treatment and those who couldn’t. Over time, the disparities expanded with shifts towards hospital beds for insured and private patients.
In one terrible example, Maltheus “Sunny” Avery, a North Carolina A & T graduate who got into a car wreck in Burlington, NC in 1950, was diagnosed with an epidermal hematoma — a clot near his brain — and sent to Duke for emergency brain surgery. But he was refused treatment due to inadequate room in the “colored” ward.
Avery was redirected to Lincoln Hospital, Durham’s Black hospital, where he died shortly after admission. Though Dr. Baker said this story quickly faded from white memory, it is something that has retained severe importance in the popular memory of Black Durhamites. This narrative is also often conflated with a similar story about Dr. Charles Drew, the Black inventor of blood banking, who died despite attempts at rescue at a white hospital in Alamance, NC. He is often misremembered as having died from the refusal of care in a racially divided South, even though he was not.
News coverage of Sunny’s death.
Duke’s first Black medical student, Delano “Dale” Meriwether, arrived the same year the hospital began desegregation, 1963, and he was the first Black M.D. in 1967. Meriwether was the only Black medical student for four years before other brave pioneers joined the school.
Dr. Tweedy reflected on his own medical school experiences at Duke during clinical rotations just a little more than 20 years ago.
“I was asked to help suture a deep gash on a Black patient’s forehead,” he said, “The patient asked if we were experimenting on him since I was still a student.” In the private clinics, he once “couldn’t go anywhere near” a white patent with a minor lesion on their arm, let alone suture that patient.
Dr. Baker said there are two narratives surrounding Duke Hospital’s desegregation. One assumes that desegregation was quick and easy and uneventful, while the other proposes that systems of racial segregation were simply transformed rather than eradicated. The latter narrative better applies to the public and private clinics that had become nearly completely racialized over time, Baker said.
Even though segregation was no longer legal, Black patients received care from less experienced medical residents in the public clinics, while white patients received care from attending physicians in the nicer, private environments.
Dr. Baker said that Duke has a complicated relationship with the community of Durham. He said the merger of Durham Regional Hospital with Duke Health in the late 1990s tapped into some long-term tensions and distrust between Duke and other medical facilities of Durham.
Public clinics versus private clinics in the hospital.
Dr. Tweedy pointed out that Duke researchers always have trouble recruiting Black patients for clinical studies, despite the fact that Durham County is about half Black and Hispanic. There is some distrust to overcome, but a diverse patient population is essential to creating robust study data that ensures that treatments will work for everyone, he said.
Medical professionals “need more than just science,” Baker concluded. He said that being trained as scientists often inclines doctors to think that they are above the larger contexts and histories they exist within, and that they can somehow remain objective.
“We have come out of specific stories and backgrounds,” Dr. Baker said. “[When we treat patients], we have to think about what story we are walking into.”
“We all carry our bags of ‘stuff'” that complicate patient prognosis and care, Dr. Tweedy concurred.
As Ann Brown (M.D., M.H.S), Vice Dean for Faculty, stated at the beginning of the conversation, “In order to move forward, we must understand where we come from.”
This is true of our nation as a whole, and Duke is certainly no exception.
Though lead has been widely eliminated from use in products due to proven health risks, the lifelong consequences of childhood lead exposure for children born in the era of lead use in gasoline are still unknown.
Aaron Reuben, fifth-year Ph.D. candidate in clinical psychology at Duke, spoke about the long-term implications of childhood lead exposure Friday, September 18th through the Nicholas School’s Environmental Health and Toxicology Seminar series. He conducts research as a member of the Moffitt and Caspi Lab, studying genes, environment, health, and behavior.
Aaron Reuben
Reuben started with a brief history of lead exposure. After the United States’ initial use of lead in gasoline in 1923, the practice became widespread with the U.S. Public Health Services approval for expansion. Five decades later, in the mid-1970s, the Environmental Protection Agency issued the first restrictions on lead use in gasoline products. Simultaneously, surveillance of population-level blood-lead levels indicated cause for concern. Though lead was phased of out of gas completely by 1995, the peak led exposures in the 70s were on average three to four times higher than current levels that demand clinical attention. Despite lead regulations, the impacts of exposure did not miraculously cease as well.
Lead use in gasoline quickly increased after its initial introduction.
The research Reuben covered in his talk centers on the Dunedin Study. This study of 1,037 people born between April 1972 and March 1973 in Dunedin, New Zealand is an ongoing longitudinal research project comprised of over 30 years of data. The cohort of participants provide a unique chance for research in which social and economic factors do not have to be detangled from findings as they represent the full range of socioeconomic statuses in their city.
Reuben’s first question was about the impact of lead exposure on psychiatric and personality differences in adulthood. Study members were asked about symptoms such as substance dependence, depression, fears and phobias, or mania. These reports were transformed into a continuous measure of general psychopathology, which indicated that children with high lead levels experienced more psychiatric problems across adulthood. Though the developmental differences were modest, the associations between lead and psychopathological issues are of a similar magnitude to other known risk factors like childhood maltreatment and family history of mental illness. Yet, unlike the latter two risk factors, Reuben said, “Lead exposure is not preordained – it’s modifiable.”
The research team also measured participant personality using the Big Five Inventory and found that individuals with high-blood level levels as children exhibited more difficult personality styles as adults. The biggest difference between groups with high and low childhood blood-lead level was the trait of conscientiousness, which has impacts on goal obtainment within one’s education and occupation, as well as overall satisfaction with relationships.
Findings from the Big Five Inventory of Dunedin participants.
The next question of the presentation centered on differences in adulthood cognitive ability. At midlife, defined as age 38 for this question, children with higher blood-lead levels had lower cognitive ability, experiencing a deficit of two IQ points per five microgram per deciliter increase of blood-lead level. Once again, though these findings were relatively modest, the loss of IQ points was accompanied by downward social mobility compared to participants’ parents. Further, when evaluations that took place at age 45 were included in the data, researchers saw even larger declines in IQ points between exposure-level groups, which Reuben predicts may even represent a trend of acceleration. He believes that as the study continues with the participants, they will find rapid decline around age 65, with higher levels of dementia symptoms among participants compared to same-aged peers.
The last question evaluated the structural integrity of the brain at midlife. The team found that children with higher lead exposure had lower gray-matter integrity, lower white-matter integrity, and older estimated brain age at age 45. Estimated brain age was predicted by an algorithm based on MRI scans, as brains look physically different as they age and gray- and white-matter integrity refers to the conditions of physical structures in the brain. These findings suggest that childhood led exposure may result in an overall lowered brain integrity at midlife, as well as accelerated brain aging.
Reuben’s take-away findings from his presentation.
Reuben’s work is important for understanding how childhood exposure to this neurotoxin has the ability to influence continued development, behavior, emotion, and life outcomes decades later. It is crucial to evaluate long-term ramifications of childhood lead exposure – a phenomena experience by hundreds of millions of people across the globe during the era of lead in gasoline who are likely unknowingly dealing with impacts now.
We are all living within the Covid moment, but we are not living within the Covid moment equally. The pandemic has exposed a recurrent rift in the United States’ healthcare system: Black Americans and other people of color (POC) are both disproportionately impacted by health issues and disproportionately lack access to care.
In a recent study on North Carolina conditions, Duke researchers found that the “odds of testing positive for [Covid] were higher for both Black and Hispanic individuals as well as within neighborhoods with a higher proportion of Black or Hispanic residents – confirming that Black and Hispanic communities are disproportionately affected.”
Panelists Keisha Bentley-Edwards (Ph.D.) and Jay Pearson (Ph.D.), moderated by Thomas Williams (J.D.)
Williams opened the panel by emphasizing the relevance of this moment: Current Covid impacts are directly informed by historical inequities and intricately span into the future. This is but one system of plaguing racism.
To speak about the intimate intersection of race and healthcare in America, Pearson offered grounding insight to systemic and structural racism. The United States is a country filled with patterns that produce and reproduce systematic advantages for those who are white while simultaneously disadvantaging people of color, most often Black and indigenous populations. Racism in America greatly transcends personal acts of racialized discrimination and harassment, he said. Racism in America is multiplex, foundational, and rooted within our society’s core.
“The U.S. national identity is tied to structural racism. …This is who we are, this is who we’ve been since the beginning of this country,” Pearson said, “The racialized inequities of Covid are simply the latest [manifestations]. We shouldn’t be surprised.”
A recently circulating figure states that 96% of people with severe outcomes or death from Covid had comorbidities, the presence of health conditions in addition to Covid. But Bentley-Edwards cautioned against misuse of this claim: “Many of these people would be alive if not for Covid.”
Though many who have died from the virus had underlying conditions, it is ultimately the virus that killed them. Communities of color often have disproportionate prevalence of underlying conditions, making them more susceptible to complications from Covid. But even when the prevalence of underlying conditions is the same among white and non-white populations, people of color are more likely to be more negatively affected by them.
For example, cardiovascular disease is similarly distributed between white and Black people, yet Black people are more likely to die of it, and at a younger age, compared to white people. Similarly, Black and other POC populations who contract Covid are more likely to die despite similar rates of contracting the virus in certain regions of the country.
Dr. Bentley-Edwards speaking during Friday’s virtual Coronavirus Conversation
Pearson and Bentley-Edwards also offered their insights on who is seen as essential and who is seen as dispensable in the United States.
Those who have been on the front lines with the most exposure and risks have been laborers who are most often under-valued Black and Brown peoples, Bentley-Edwards said. Though Covid terminology has come to dub them essential, it is undeniable that our society continues to see these types of workers as dispensable or replacable, and thus does not protect the people responsible for protecting us. Because many people of color live in multi-generational households as a culturally protective factor, increased chance of contracting Covid has led to uncertainties on the safety of returning home to young and elderly family members, she said. Further, the disproportionate unemployment rate of 13% for Black Americans compared to the 8.4% national rate is a staggering one. Since insurance is tied to employment, Black and Brown communities often avoid treatments due to the financial burden of unaffordable and inaccessible care.
Within the pandemic, we have seen the ever-present epidemiological impacts of police brutality and murder in the U.S with fresh eyes, the panelists said. In many ways, Black peoples’ experiences with healthcare mirrors that of their experiences with police – likely because both systems are anchored by an unjust nucleus.
“[Covid and police brutality] are slightly different manifestations of the same phenomenon,” Pearson said. We are able to easily identify the murders of individuals such as Breonna Taylor, George Floyd, and Ahmaud Arbery as stolen lives due to racist actions, however the slow burn of a racist health care system is less easily conceptualized or reconciled with, he said. Either way, the cause is one and the same.
Racism within systems that are meant to protect have generated a deep mistrust from Black and Brown people. Williams brought up the issue of a potential Covid vaccination amongst communities of color. “You have to know the history and why they would hesitate,” Bentley-Edwards said, bringing up the Tuskegee experiments and the work of J. Marion Sims. These accounts offer grim revelation of a heinous, racist history of exploiting vulnerable people for scientific and medical explorations.
Bentley-Edwards said that governments and healthcare institutions must address the rightful apprehensions of Black and Brown people in order to decrease vaccine hesitancy and serve at-risk communities. “What are they going to do differently?”
Williams also proposed the notion of data collection as a source of bias: In what ways are the data informatics that are collected reflections of an inequitable system? Bentley-Edwards and Pearson both suggest that to understand the current moment, as well as the healthcare system more largely, there needs to be collection and analysis of racial data. Additionally, there simply needs to be measurements for indicators beyond conventional ones which do not properly account for impacts on communities of color.
The push for new and different kind of data is supported by a growing evidence for the manifestations of inequality within biological bodies. For example, Pearson spoke about his own research on telomeres, a protective structure on the ends of chromosomes that protect DNA from degradation. Telomeres are telling both of stress and aging. Pearson’s work found that the average Black American woman is six to seven biological years older than a white American woman of the same age by evaluating telomere lengths, controlling for income, education, and other important socioeconomic factors. This indicates physiological affects linked to the stresses and disproportionalities of race down to the cellular level. Through genetics, mental health, and other physical degradations, the impacts of racism and racist healthcare quite literally last a lifetime and are even intergenerational.
Diagram of telomere from a study conducted by Dr. Pearson
Pearson closed the panel by urging attendees to take action where they find themselves. Though the need for animated policy which reflects recent discussions and protests is dire, the local spaces we find ourselves in need to be reshaped as well – including our universities.
In this moment, our responsibilities to one another have become more obvious than ever before. We must become more adept in thinking about and taking action for the communities in which we live and are connected to, whether they are comprised of people who look like us or not.
Imagine: you wake on a chilly November morning, alarm blaring, for your 8:30 am class. You toss aside the blankets and grab your phone. Shutting the alarm off reveals a Washington Post notification. But this isn’t your standard election headline. You almost drop your phone in shock. It can’t be, you think. This is too good to be true. It’s not — a second later, you get a text from the SymMon app, notifying you of your upcoming appointment in the Bryan Center.
A vaccine for COVID-19 is finally available, and you’re getting one.
This scenario could be less far-fetched than one might think: the Centers for Disease Control and Prevention has told officials to prepare for a vaccine as soon as November 1st. To a country foundering due to the economic and social effects of COVID-19, this comes as incredible news — a bright spot on a bleak horizon. But to make a vaccine a reality, traditional phase 3 clinical trials may not be enough. What are challenge trials? Should they be used? What’s at stake, and what are the ethical implications of the path we choose?
Dr. Marc Lipsitch, Director of the Center for Communicable Disease Dynamics at the Harvard School of Public Health, began by comparing traditional phase 3 trials and challenge trials.
In both kinds of trials, vaccines are tested for their “safety and ability to provoke an immune response” in phases 1 and 2. In phase 3 trials, large numbers (typically thousands or tens of thousands) of individuals are randomly assigned either the vaccine being tested or a placebo. Scientists observe how many vaccinated individuals become infected compared to participants who received a placebo. This information enables scientists to assess the efficacy — as well as rarer side effects — of the vaccine.
Marc Lipsitch
In challenge trials, instead of random assignment, small numbers of low-risk individuals are deliberately infected in order to more directly study the efficacy of vaccine and treatment candidates. Though none are underway yet, the advocacy group 1Day Sooner has built a list of more than 35,000 volunteers willing to participate.
Dr. Cameron Wolfe, an Infectious Disease Specialist, Associate Professor of Medicine, and Clinical Expert In Respiratory and Infectious Disease at the Duke Medical School, provided an overview of the current vaccine landscape.
Cameron Wolfe
There are currently at least 150 potential vaccine candidates, from preclinical to approved stages of development. Two vaccines, developed by Russia’s Gamelaya Research Institute and China’s CanSinoBIO, have skipped phase 3, but are little more than an idiosyncrasy to Dr. Wolfe, as there is “minimal clarity about their safety and efficacy.” Three more vaccines of interest — Moderna’s mRNA vaccine, Pfizer’s mRNA vaccine, and Oxford and AstraZeneca’s adenovirus vaccine — are all in phase 3 trials with around 30,000 enrollees. Scientists will be watching for a “meaningful infection and a durable immune response.”
Dr. Nir Eyal, the Henry Rutgers Professor of Bioethics and Director of The Center for Population-Level Bioethics at Rutgers University, explained how challenge trials could fit into the vaccine roadmap.
According to Dr. Eyal, challenge trials would most likely be combined with phase 3 trials. One way this could look is the use of challenge trials to weed out vaccine candidates before undergoing more expensive phase 3 trials. Additionally, if phase 3 trials fail to produce meaningful results about efficacy, a challenge trial could be used to obtain information while still collecting safety data from the more comprehensive phase 3 trial.
Nir Eyal
Dr. Eyal emphasized the importance of challenge trials for expediting the arrival of the vaccine. According to his own calculations, getting a vaccine — and making it widely available — just one month sooner would avert the loss of 720,000 years of life and 40 million years of poverty, mostly concentrated in the developing world. (Dr. Eyal stressed that his estimate is extremely conservative as it neglects many factors, including loss of life from avoidance of child vaccines, cancer care, malaria treatment, etc.) Therefore, speed is of “great humanitarian value.”
Dr. Wolfe added that because phase 3 trials rely on a lot of transmission, if the US gets better at mitigating the virus, “the distinction between protective efficacy and simple placebo will take longer to see.” A challenge study, however, is “always a well defined time period… you can anticipate when you’ll get results.”
The panelists then discussed the ethics of challenge trials in the absence of effective treatment — as Krawiec put it, “making people sick without knowing if we can make them better.”
Dr. Wolfe pointed to the flu, citing challenge trialsthat havebeen conducted even though current treatments are not uniformly effective (“tamiflu is no panacea”). He then conceded that the biggest challenge is not a lack of effective therapies, but the current inability to “say to a patient, ‘you will not have a severe outcome.’ It varies so much from person to person, I guess.” (See one troubling example of that variance.)
Dr. Eyal acknowledged the trouble of informed consent when the implications are scarcely known, but argued that “in extraordinary times, business as usual is no longer the standard.” He asserted that if people volunteer with full understanding of what they are committing to, there is no reason to assume they are less informed than when making other decisions where the outcome is as yet unknown.
Dr. Lipsitch compared this to the military: “we are not cheating if we cannot provide a roadmap of future wars because they are not yet known to us.” Rather, we commend brave soldiers (and hope they come home safe).
Furthermore, Dr. Eyal asserted that “informed consent is not a comprehensive understanding of the disease,” lest much of the epidemiological research from the 1970s be called into question too. Instead, volunteers should be considered informed as long as they comprehend questions like, “‘we can’t give you an exact figure yet; do you understand?’”
Agreeing, Dr. Wolfe stated that when critics of challenge trials ask, isn’t your mission to do no harm?, he asks, “Do no harm in regards to whom?” “Who is in front of you matters,” Dr. Wolfe confirmed, “that’s why we put up safeguards. But as clinicians it can be problematic [to stop there]. It’s not just about the patient, but to do no harm in regards to the broader community.”
The experts then discussed what they’d like to see in challenge trials.
Dr. Wolfe said he’d like to see challenge trials carried out with a focus on immunology components, side effect profiles, and a “barrage” of biological safety and health standards for hospitals and facilities.
Dr. Eyal stated the need for exclusion criteria (young adults, perhaps age 20-25, with no risk factors), a “high high high” quality of informed consent ideally involving a third party, and access to therapies and critical care for all volunteers, even those without insurance.
Dr. Lipsitch stressed the scientific importance of assessing participants from a “virological, not symptom bent.” He mused that the issue of viral inoculum was a thorny one — should scientists “titrate down” to where many participants won’t get infected and more volunteers will be needed overall? Or should scientists keep it concentrated, and contend with the increased risk?
Like many questions pondered during the hour — from the ideal viral strain to use to the safest way to collect information about high risk patients — this one remained unanswered.
So don’t mark November 1st on your calendar just yet. But if you do get that life-changing notification, there’s a chance you’ll have human challenge trials to thank.
Like nearly all other aspects of life, the normal routines of Duke research labs came to a grinding halt due to COVID-19. Duke researchers shared their reflections on the struggles and insights the process of research shutdown and reboot has had within their labs during a Virtual Research Town Hall on Thursday, September 3rd.
Larry Carin (Ph.D.)
Collin S. Duckett (Ph.D.)
Jamie R. Privratsky (MD, Ph.D.)
Debra Silver (Ph.D.)
Anne West (Ph.D.)
Virtual Research Town Hall Panelists
The Town Hall, titled “The Impact of COVID 19 on Research at Duke, Overcoming Challenges and Pressures” was moderated by Duke Vice President for Research, Larry Carin (Ph.D.). Dr. Carin mentioned that discussion of shutting down the research enterprise began in February, and at that point in time it seemed nearly hysterical. However, by mid-March shut-down plans were fully in progress, leaving labs out of commission until mid-June. To get research at Duke back underway, labs were forced to significantly reduce the density of people in facilities and no undergraduate students were allowed to participate.
Though most of the basic science labs are back in operation now, human subjects research trials have had a slower return. In no way is it business as usual. Detailed planning and scheduling, a focus on social distancing, and daily health surveys are all part of the new normal. “There is almost a Big Brother feel to this,” Dr. Carin said, comparing the moderated tracking of who enters facilities through their DukeCard swipes to George Orwell’s 1984 dystopian society.
Associate Professor Debra Silver Ph.D. spoke about her neurodevelopmental lab in molecular genetics and microbiology (MGM). In the three-month shutdown, lab members focused on writing reviews, grants, manuscripts, and took online classes to improve skills. Since re-opening, Silver’s lab has implemented lab shifts, pre-scheduled experiments, and coordinated use of shared equipment. Some of the biggest issues are the trainees missing out on critical networking and undergraduates forced to transition to nearly exclusively online work. Silver also voiced serious concern for the mental and physical health of lab members, logistical coordination of childcare and homeschooling, challenges faced by international trainees, and the need for flexibility. However, there were some silver linings as well. The Silver Lab engaged with lots of seminars, had joint lab meetings, and the mutual support for one another grew immensely under the unique circumstances.
Dr. West points out the enduring emotional impacts of COVID.
Both Silver’s lab and the West Lab, led by professor Anne West Ph.D. in neurobiology, are heavily reliant on mice for wet lab work. The mandates to reduce their mouse colonies by more than 50% was a large task and now that the labs are up and running, re-expanding the colonies has been a primary focus. West said that, similar to the Silver Lab members, half of her team picked up writing or a computational project while the other half attended online classes or meetings during shutdown. Undergraduates read and presented research papers – which turned out to be a very fruitful training experience.
One major roadblock for the West Lab’s reopening were the murders of George Floyd, Breonna Taylor, and Ahmoud Arbery. The civic unrest surrounding these deaths and the revivalism of the Black Lives Matter movement became a frequent point of discussion in lab meetings. Some members of the West Lab were unable to work during this time. West emphasized the importance of lowered expectations. She asked everyone to focus on one core experiment and to try to come into the lab for at least a few hours a day, a few days a week. The lab has been gaining traction with new data and research papers nearing completion. Like other panelists, West discussed prevailing issues including anxiety and depression, continued societal uncertainties, and the questionable financial future for research.
Assistant professor of anesthesiology Jamie R. Privratsky MD, Ph.D. highlighted COVID’s impact on clinical and critical care research. Among the positive impacts are the Society of Critical Care Medicine’s COVID-19 registry database, the abilities to do observational and database research work, and research opportunities for working with COVID patients. However, the rest of critical care research has been completely sidelined, clinician-scientists have been moved to mostly clinical duties, and there have been lots of administrative hurdles for conducting COVID related research.
A slide from Dr. Pivratsky’s presentation.
Many colleagues share Dr. Privratsky’s mixed thoughts on the gains and losses during the halt of critical care research. For those who were able to conduct some research, the risks to personal health also posed looming anxiety and danger. Dr. Privratsky chose to do what he could being physically away from his lab and worked to update protocols, maintain electronic lab notebooks, write methods sections of papers, and care for his mouse colony. He also submitted three grant proposals and said that he left the shutdown with a clearer vision and direction for his research.
The School of Medicine’s Vice Dean for Basic Science, Colin S. Duckett Ph.D. closed the town hall with encouraging reflections. Out of 17,000 Duke administered COVID tests, there have been very few positives. Duckett emphasized how seriously the Duke community and its recently returned students are taking the continued threat of Coronavirus. Though communications persist as a challenge and many argue that life right now just doesn’t feel right, Duckett called attendees’ attention to the fact that the research enterprise was successfully ramped down, ramped back up, and lab activities have made a nearly completely return. This was and continues to be no small feat and is possible due to highly collaborative efforts, he said.
Good news from Dr. Duckett about the state of Duke’s research enterprise.
Further, there were large insights gleaned from this collective experience; those of researchers’ resiliency, the importance of community, and the need to look beyond work and check in on each other as human beings. Research and the people who make it possible do not exist in a vacuum away from society. Their work and their well-being are subject to the pandemic just like everyone else. Yet, similar to the broader global public, researchers and their research are emerging stronger than before in the face of COVID-19.
TikTok’s illicit collection of user data recently drew fire from US officials. But TikTok’s base—largely young adults under 25—was unfazed. In viral videos posted in July and August, users expressed little concern about their digital privacy.
“If china wants to know how obsessed i am with hockey,” wrote one user, “then just let them its not a secret.” “#Takemydata,” captioned another, in a video racking up 6,000 likes and over 42,000 views.
As digital technologies become ever more pervasive – or even invasive – concerns for privacy should be a concern, a pair of experts said in a Duke Science & Society webinar earlier this month.
TikTok and digital marketing aside, data collection can have real, tangible benefits. Case in point: COVID-19. Researchers at Duke and elsewhere are using peoples’ fitness trackers and smart watches to try to understand and predict the pandemic’s spread by monitoring a variety of health metrics, producing real-time snapshots of heart rate, blood pressure, sleep quality, and more. Webinar speaker Jessilyn Dunn of Duke biomedical engineering and her team have tapped into this data for CovIdentify, a Duke-funded effort to predict COVID infections using data collected by smartphones and wearable devices.
Health data from smartphones and fitness trackers may help predict and identify disease.
For several years, Dunn’s lab has researched digital biomarkers of disease—that is, how health data collected by tech we carry every day can predict anything from heart disease to cognitive decline.
It’s a potential goldmine: One recent poll suggests that 40 million Americans own some kind of smartwatch or fitness tracker. And the wearables market is rapidly expanding—by 2022, it may be worth upwards of 25 billion dollars.
As coronavirus cases began to rise in the US, Dunn’s lab quickly pivoted to develop COVID-specific biomarkers. “We have these devices … that perform physiologic monitoring,” Dunn said, “This is a method of taking vitals continuously to try to monitor what’s going on with people.”
Say you’re a participant in Dr. Dunn’s study. You download the CovIdentify app, which analyzes health data collected by your phone or smartwatch. Short daily surveys then assess your exposure to COVID-19 and whether you’ve developed any symptoms. Dunn and her team hope to find a link, some specific change in vitals that corresponds to COVID-19 infection.
There are some challenges. CovIdentify must account for variability between devices—data collected from a Fitbit, for example, might differ dramatically from an Apple Watch. And because COVID-19 manifests in unique ways across populations, a truly universal biomarker may not exist.
However, panelist Marielle Gross—a bioethicist at the University of Pittsburgh—said projects like Dunn’s raise questions of digital privacy. Gross emphasized how easily our health data can be abused.
Left: Jessilyn Dunn, PhD, a professor at Duke University and CovIdentify Researcher Right: Marielle Gross, MD, MBE, a bioethicist and professor at the University of Pittsburgh
“Digital specimen is the digital representation of the human body,” she said. “Disrespecting it disrespects the body it represents.”
Dr. Gross cited South Korea’s efforts to curb COVID-19 as a cautionary tale. As part of the government’s response, which quickly minimized cases early in the pandemic, exposed or infected South Koreans were expected to stay home and isolate, tracked using GPS-enabled devices.
But many South Koreans chose to leave their devices at home, rather than be tracked by their government. In response, the government required its citizens to carry their devices, 24/7. In a pandemic, desperate measures may be called for. But, Gross suggests, it isn’t hard to imagine a grimmer future—where the government requires all citizens to share their location, all the time.
Gross argues that we must fundamentally shift how we think about our personal data. “There’s this broad assumption that we have to give up privacy to reap the benefits of collective data.” Gross noted. “And that’s false.”
Most ‘digital natives’ aren’t naive. They’re well aware that internet companies collect, analyze, and sell their data, sometimes to malicious effect. But many view data collection as a necessary tradeoff for an intuitive and tailored web experience.
So where do we go from here? Dr. Gross points to new developments like zero knowledge proofs, which use complex algorithms to verify data without actually seeing it. This technique promises anonymity without compromising the value of collective data. And as computing power increases, it may also be possible to perform real-time analysis without ever transmitting or storing collected health data.
And for future tech? In Dr. Gross’s opinion, ethical implications must be considered from day one. “Those sorts of considerations are not the kind of thing that you can tack on later. They have to be built into devices…at the ground floor.”
Millions of data points. Ten weeks. Three Duke undergraduates. Two faculty facilitators. One project manager and one pretty cool data visualization website.
Undergraduates Katherine Cottrell (’21), Michaela Kotarba (’22) and Alexander Burgin (’23) spent the last two and a half months looking at changes in Duke’s student body enrollment over the last 50 years. The cohort, working with project manager Anna Holleman, professor Don Taylor and university archivist Valerie Gillispie, used data from each of Duke’s colleges spanning back to 1970. Within the project, the students converted 30 years of on-paper data to machine-readable data which was a hefty task. “On Being a Blue Devil” presented their final product during a Zoom-style showcase Friday, July 31: An interactive data-visualization website. The site is live now but is still being edited as errors are found and clarifications are added.
The cover page of the launched interactive application.
The team highlighted a few findings. Over the last 20 years, there has been a massive surge in Duke enrollment of students from North Carolina. Looking more closely, it is possible that grad enrollment drives this spike due to the tendency for grad students to record North Carolina as their home-state following the first year of their program. Within the Pratt School of Engineering, the number of female students is on an upward trend. There is still a prevalent but closing gap in the distribution between male and female undergraduate engineering enrollment. A significant drop in grad school and international student enrollment in 2008 corresponds to the financial crisis of that year. The team believes there may be similar, interesting effects for 2020 enrollment due to COVID-19.
However, the majority of the presentation focused on the website and all of its handy features. The overall goal for the project was to create engaging visualizations that enable users to dive into and explore the historic data for themselves. Presentation attendees got a behind-the-scenes look at each of the site’s pages.
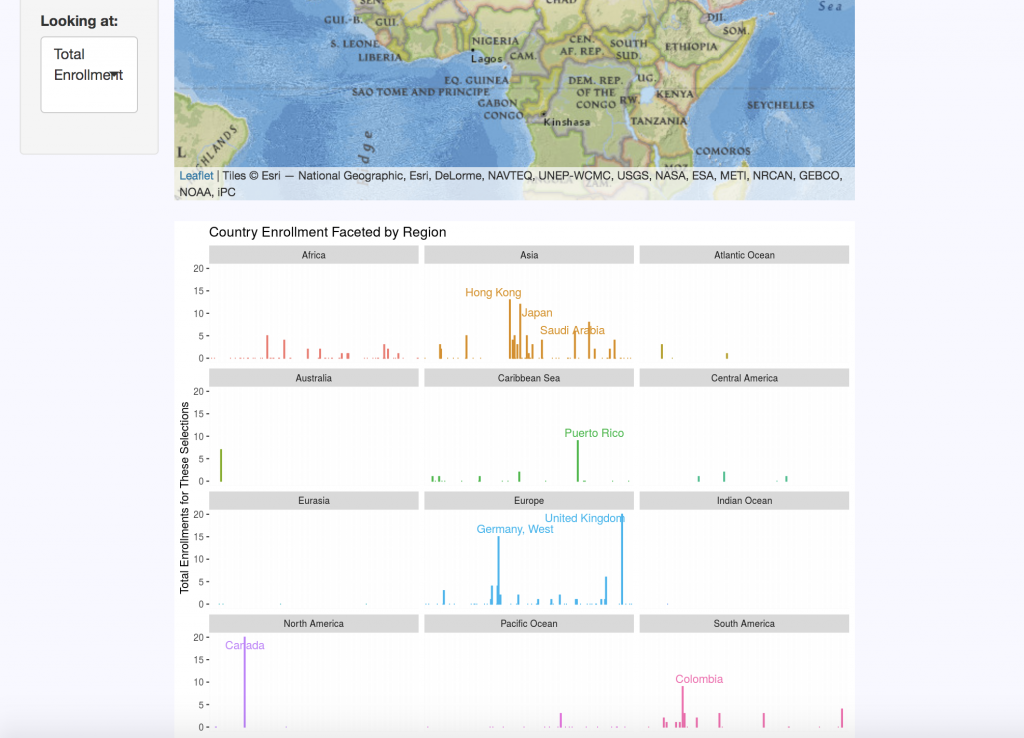
Breakdown of enrollment by region within different countries outside of the United States.
The “Domestic Map” allows website visitors to select the school, year, sex, semester, and state they wish to view. The “International Map” displays the same categories, with regional data replacing state distributions for international countries. Each query returns summary statistics on the number of students enrolled per state or region for the criteria selected.
A “Changes Over Time” tab clarifies data by keeping track of country and territory name changes, as well as changes in programs over the five decades of data. For example, Duke’s nursing program data is a bit complicated: One of its programs ended, then restarted a few years later, there are both undergraduate and graduate nursing schools, and over a decade’s worth of male nursing students are not accounted for in the data sets.
The “Enrollment by Sex” tab displays breakdown of enrollment using the Duke-established binary of male and female categories. This data is visualized in pie charts but can also be viewed as line graphs to look at trends over time and compare trends between schools.
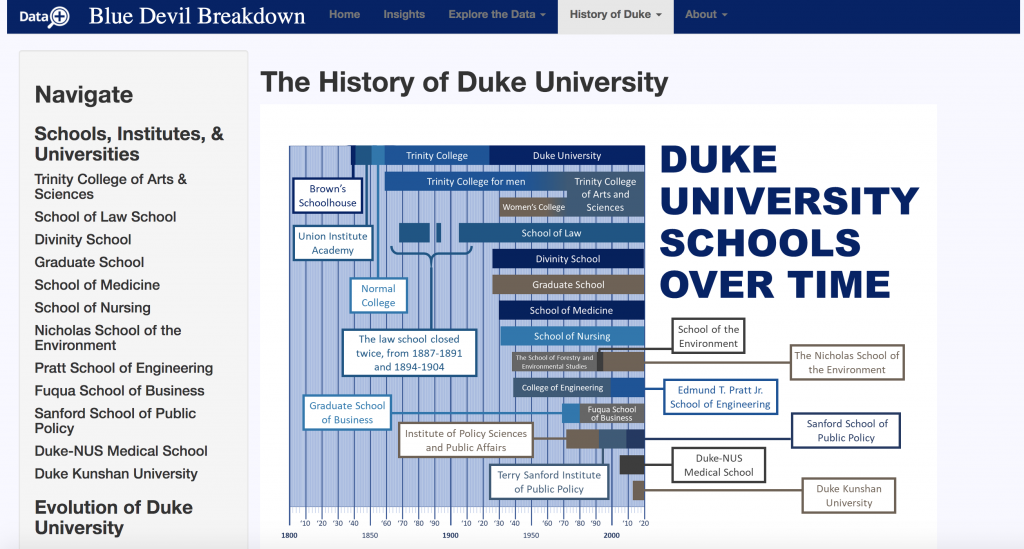
“History of Duke” offers an interactive timeline that contextualizes the origins of each of Duke’s schools and includes a short blurb on their histories. There are also timelines for the history of race and ethnicity at Duke, as well as Duke’s LGBTQ history. Currently, no data on gender identity instead of legal sex was made available for the team. This is why they sought to contextualize the data that they do have. If the project continues, Cottrell, Kotarba, and Burgin strongly suggest that gender identity data be made accessible and included on the site. Racial data is also a top priority for the group, but they simply did not have access to this resource for during the duration of their summer project.
Timeline of Duke’s various schools since it was founded in the 1830’s.
Of course, like most good websites, there is an “About” section. Here users can meet the incredible team who put this all together, look over frequently asked questions, and even dive deeper into the data with the chance to look at original documents used in the research.
From left to right: Project lead Don Taylor (Ph.D), project lead Valerie Gillispie, and project manager Anna Holleman
Each of the three undergrads of the “On Being a Blue Devil” team gained valuable transferable skills – as is a goal of Duke’s Data+ program. But the tool they created is likely to go far beyond their quarantined summer. Their website is a unique product that makes data fun to play with and will drive a push for more data to be collected and included. Future researchers could add many more metrics, years, and data points to the tool, causing it to grow exponentially.
Many Duke faculty members are already vying for a chance to talk with the team about their work.