By Pranali Dalvi
 Cancer is the uncontrolled growth of cells. We take this idea for granted today, but the definition of cancer evaded us for many years.
Cancer is the uncontrolled growth of cells. We take this idea for granted today, but the definition of cancer evaded us for many years.
In a talk on on Dec. 6, the Pulitzer Prize-winning author, physician, and cancer researcher Dr. Siddhartha Mukherjee, took his audience on a journey through the archives of medicine to build a bird’s eye view of cancer and how we define the disease today. The presentation was part of the Weaver Memorial Lecture, hosted every other year in memory of William B. Weaver, a 1972 Duke graduate.
“The entire history of our encounter with cancer really consists of four major discoveries, of which we’re experiencing and living the fourth,” Mukherjee said.
Phase I: A Disease of Cells
The first discovery was that cancer is a disease of cells. In the late 1800s, the idea that cancer is a dysregulated growth of our own cells was a deeply radical idea. Scientists at the time and earlier insisted that all diseases in the human body could be explained by either an excess or a deficit in one of four fluids – black bile, yellow bile, blood and phlegm. Making no exception, Roman physician Galen posited that cancer, too, resulted from an excess of black bile in the body.
Andreas Vesalius, the founder of modern human anatomy, overthrew Galenic tradition by disproving the existence of black bile, which forced surgeons and early cancer scientists to seek a different explanation for cancer. That explanation came from Rudolf Virchow, who examined cancerous tissue microscopically and realized that all cancers had a commonality – the overabundance of cells. This conception of cancer drew in surgeons: if cancer originated from a single cell, it could be eliminated by surgically removing the cancerous cluster.
Scientists also developed radiation therapy to destroy cancer. Unfortunately, many who received radiation therapy for cancer ended up contracting cancer. Biologists were perplexed: how could X-rays which killed cells also be responsible for the abnormal growth of cells in cancer? Was there an interaction via the environment that was inducing cancer in cells? This question remained a mystery for over 70 years.
Another way to kill cells was chemotherapy, which emerged when mustard gas, a war gas, was found. Scientists added it to their arsenal of surgical and radiation treatment for cancer.
Phase II: A Disease of Genes
Still, these cancer treatments were all empirical; scientists had no biological understanding of the mechanism of the disease. They hypothesized that the empirical strategy in conjunction with chemotherapy, radiation, and surgery would bring a cure to all cancers by the summer of 1979. However, that summer came and went, forcing scientists to explore the mechanism of cancer before planning their next attack.
“The number of cancers diagnosed increased at the same time the number of deaths [due to emerging treatments] decreased, creating a cancer society – a society in which cancer became more visible in our public consciousness,” Mukherjee said.
The increased presence of cancer pressed for a mechanistic understanding of cancer at the gene level. The idea, first proposed in 1976, that cancer was a disease of genes was revolutionary yet disappointing. People had hoped that cancer was a virus or something foreign but the idea that cancer was in our own cells was terrifying – the enemy was our own body.
Phase III: A Disease of Genomes

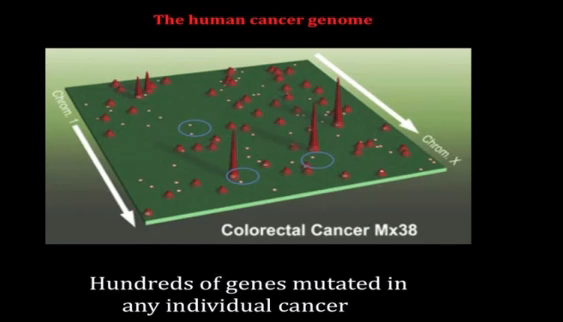
The tall peaks in this map of human prostate cancer represent genes commonly mutated in cancer. The smaller peaks are rarely mutated genes, and the small dots are genes mutated in a single cancer patient. Credit: Johns Hopkins University.
In 1990, the definition of cancer changed once again as it was discovered to be a disease of genomes. Not just one gene but many genes are mutated in cancer, a depiction of the disease painted by the work of
Bert Vogelstein among others. As multiple genes in our genome regulate normal cells, multiple genes must be mutated to cause cancerous cells.
While some genes are mutated in cancer patients across the board, there are mutations unique to each individual, too. The problem is that the tumors look identical under the microscope. Mukherjee compares this phenomenon to the fact that every single human face has a common anatomy but is still quite different.
“The challenge as you sequence cancer genomes is that there is great diversity and therefore you reach the frightening corollary that every breast cancer is unique in the same way that every woman who has breast cancer is unique,” Mukherjee said.
With such variation, how do we remain optimistic about a cure?
Mukherjee offered acute promyelocytic leukemia (APL) as an example. Once known as the most threatening variant of acute leukemias, APL is now the most curable variant. One gene was identified that was common to all APL variants and one medicine – retinoic acid – was successful in treating this disease.
Phase IV: An Organismal Disease
As of 2010, cancer has been reconceived as an organismal disease: the human is simultaneously the site of the cancer, its prevention, and cure.
“Our next step is to understand the physiology of cancer – not just the cell biology, not the gene biology, nor the genome biology – but the physiology of cancer,” Mukherjee reminded us.
Despite the disease’s high level of complexity, scientists have new tools of computation to process data they previously could not, leading to the belief that cancer is a pathway disease. It’s not just genes and genomes that are mutated in cancer, it’s the cells’ language that drives those pathways and the resulting abnormalities. That language is the focus of scientists new cancer investigations and another piece of the devastating disease’s biography.